
How Long Does Ovarian Reserve Respond to Supplements? A Doctor’s Complete Guide
Introduction
One of the most common and emotionally charged questions I hear in clinical practice is: “Doctor, how long will it take for my ovarian reserve to improve if I start supplements?” Women diagnosed with low AMH, diminished ovarian reserve (DOR), or those preparing for IVF often search desperately for ways to improve fertility outcomes. This brings us to the key question: how long ovarian reserve responds to supplements, and what kind of improvement is realistically possible.
It is important to clarify early—supplements do not create new eggs. A woman is born with a fixed number of eggs. However, what supplements can influence is egg quality, mitochondrial function, hormonal environment, and follicular responsiveness, which directly affect fertility success, IVF outcomes, and pregnancy chances.
In this detailed guide, I will explain the scientific timeline, expected changes, best supplements, lifestyle support, and common myths—based on medical evidence and real-world fertility practice.
1. What Is Ovarian Reserve?
Ovarian reserve refers to the quantity and quality of eggs remaining in a woman’s ovaries. While quantity declines steadily with age, quality declines due to genetic instability, oxidative stress, and mitochondrial aging.
A woman may have:
- Normal egg number but poor egg quality
- Low egg number but reasonable quality
- Both low quantity and quality
Understanding this distinction is crucial when discussing supplementation.
Key Markers of Ovarian Reserve
Doctors assess ovarian reserve using:
- AMH (Anti-Müllerian Hormone): Reflects remaining follicle pool
- Antral Follicle Count (AFC): Ultrasound count of resting follicles
- FSH & Estradiol (Day 2–3): Indirect ovarian response markers
Supplements mainly influence egg quality and follicle health, which may secondarily affect AMH or AFC in some women.
2. Can Ovarian Reserve Really Improve?
From a strict biological perspective:
- ❌ Egg number cannot increase
- ❌ Menopause cannot be reversed
- ❌ Genetic ovarian aging cannot be stopped
However:
- ✅ Egg quality can improve
- ✅ Follicle survival can improve
- ✅ Ovarian response to stimulation can improve
- ✅ IVF outcomes may improve even without AMH rise
This is why understanding how long ovarian reserve responds to supplements requires looking beyond lab numbers alone.
3. Why Supplements Are Used for Low Ovarian Reserve
Biological Rationale
Egg cells (oocytes) are the largest cells in the human body and contain thousands of mitochondria. As women age:
- Mitochondrial energy production declines
- Oxidative stress increases
- DNA repair weakens
Supplements aim to:
- Improve mitochondrial ATP production
- Reduce oxidative damage
- Enhance hormonal signaling
- Improve follicular microenvironment
Who Benefits Most From Supplements?
Women most likely to benefit include:
- Low AMH or DOR patients
- Women over 35 years
- IVF poor responders
- Women with recurrent IVF failure
- PCOS patients with poor egg quality
Patients with extremely low reserve may still benefit in egg quality, even if AMH does not rise.
4. The Egg Development Timeline
One of the most misunderstood facts in fertility medicine is how long egg maturation takes.
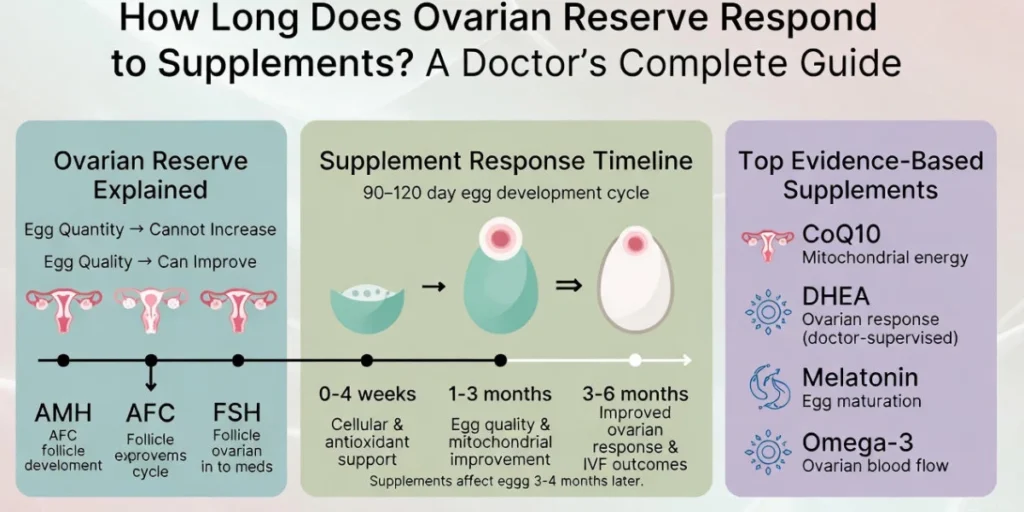
➡️ A single egg takes 90–120 days to develop from a resting follicle into an ovulatory egg.
This means:
- Supplements taken today affect eggs 3–4 months later
- Immediate changes are biologically impossible
- Short-term use leads to disappointment
This follicular timeline explains why ovarian reserve responds slowly to supplements.
General Timeline of Response
Based on clinical evidence and practice:
| Time Period | What Happens |
| 0–4 weeks | Internal biochemical and antioxidant effects |
| 1–3 months | Egg quality and mitochondrial improvement |
| 3–6 months | Possible AMH stabilization or mild increase |
| 6+ months | Maintenance or plateau phase |
Most doctors recommend at least 3 months before evaluating response.
When Do Tests Start Changing?
- AMH: May show slight rise after 3–6 months in some women
- AFC: May stabilize or improve marginally
- IVF Outcomes: Often improve before lab values change
This is why focusing only on AMH can be misleading.
5. Timeline by Individual Supplements
5.1 Coenzyme Q10 (Ubiquinol)
Mechanism:
Improves mitochondrial energy production in oocytes.
Response Timeline:
- Egg quality improvement: 8–12 weeks
- IVF response: 3–4 months
Clinical Benefit:
- Better embryo quality
- Reduced chromosomal abnormalities
CoQ10 is one of the most researched fertility supplements.
5.2 DHEA
Who Should Use It:
- Women with DOR or low AFC
- IVF poor responders
(Not recommended without medical supervision)
Timeline:
- Hormonal response: 6–8 weeks
- IVF outcome improvement: 3–4 months
DHEA may slightly increase AMH in select patients but works mainly by improving ovarian response.
5.3 Myo-Inositol & D-Chiro Inositol
Best For:
- PCOS
- Insulin resistance
- Ovulatory dysfunction
Timeline:
- Hormonal balance: 4–8 weeks
- Ovulation improvement: 2–3 months
Indirectly improves egg quality through metabolic regulation.
5.4 Antioxidants (Vitamin C, E, ALA)
Role:
- Reduce oxidative stress
- Protect DNA integrity
Timeline:
- Cellular protection begins early
- Egg quality benefits: 2–3 months
5.5 Omega-3 Fatty Acids
Benefits:
- Improved ovarian blood flow
- Reduced inflammation
Timeline:
- Follicular environment improvement: 8–12 weeks
5.6 Melatonin
Unique Role:
- Improves egg maturation
- Protects spindle formation
Timeline:
- IVF egg quality improvement: 2–3 months
6. Expected Changes: What Supplements CAN Improve
- Egg quality
- Embryo quality
- IVF response
- Fertilization rates
- Pregnancy outcomes
Many women conceive without any AMH rise, proving that egg quality matters more.
What Supplements CANNOT Reverse
- Ovarian aging
- Menopause
- Genetic egg depletion
This distinction prevents unrealistic expectations.
7. Factors That Affect How Fast Ovarian Reserve Responds
- Age: Younger women respond faster
- Baseline AMH: Moderate reserve responds better
- BMI: Obesity delays response
- Smoking: Severely reduces benefit
- Vitamin D deficiency: Blunts AMH response
- Stress & sleep: Affect hormonal signaling
Addressing these improves supplement effectiveness.
8. Supplements vs IVF: Timing Strategy
8.1 When to Delay IVF for Supplements
- Borderline AMH
- First IVF attempt
- Younger women (<38 years)
A 3-month optimization period may improve outcomes.
8.2 When NOT to Delay IVF
- Very low AMH (<0.5)
- Age >40 years
- Time-sensitive fertility cases
In such cases, supplements should run alongside IVF, not delay it.
8.3 Combined Approach
Most fertility specialists now recommend:
- Supplements + IVF stimulation
- Continued use through egg retrieval
This approach maximizes egg competence.
9. Lifestyle Changes That Enhance Supplement Response
- Anti-inflammatory fertility diet
- Avoid smoking and alcohol
- Moderate exercise
- Stress reduction techniques
- Adequate sleep (7–8 hours)
- Avoid endocrine-disrupting chemicals
Lifestyle optimization can double the effectiveness of supplements.
Doctor’s Clinical Experience & Real-World Outcomes
In clinical practice:
- Egg quality improves before lab numbers
- Most patients feel discouraged too early
- Short-term supplement use is the biggest mistake
Patients who commit to 3–6 months consistently have better outcomes, even with low AMH.
For patient education tools and fertility calculators, I often recommend resources from
👉 https://erectileandfertilityguide.com to track fertility parameters and understand realistic expectations.
Conclusion
The honest medical answer is 3 to 6 months, depending on age, baseline reserve, supplement choice, and lifestyle factors. Supplements do not increase egg count, but they can significantly improve egg quality, ovarian responsiveness, and fertility outcomes when used correctly and patiently.
Success comes from realistic expectations, medical supervision, and consistency—not miracle promises.
FAQs; How Long Does Ovarian Reserve Respond to Supplements
- How long does ovarian reserve respond to supplements before IVF?
Based on clinical experience, how long does ovarian reserve respond to supplements depends on the egg maturation cycle. Most women require at least 3 months of consistent supplementation before IVF to see improvements in egg quality, even if AMH levels remain unchanged. - Can supplements really increase AMH levels?
AMH may increase slightly in some women, but fertility improvement can occur without a measurable AMH rise. When patients ask how long does ovarian reserve respond to supplements, I emphasize that improved egg competence is more important than AMH numbers alone. - What is the minimum time to take supplements for egg quality improvement?
The minimum recommended duration is 90 days, which aligns with the ovarian follicle development process. This timeframe explains how long does ovarian reserve respond to supplements from a biological standpoint. - Which supplement works fastest for ovarian reserve support?
Among commonly used options, CoQ10 and melatonin show egg quality benefits within 2–3 months. However, understanding how long does ovarian reserve respond to supplements requires realistic expectations rather than quick results. - Can ovarian reserve improve after 40 with supplements?
While egg quantity cannot increase after 40, egg quality and IVF response may improve. Many women ask how long does ovarian reserve respond to supplements at this age, and the answer remains the same—around 3–6 months for potential benefit. - Should I repeat AMH testing after taking supplements?
Yes. AMH should be repeated after 3–6 months, not earlier. Testing too soon does not reflect how long does ovarian reserve respond to supplements accurately. - Are fertility supplements safe for long-term use?
Most antioxidants and micronutrients are safe when properly dosed. However, DHEA and hormonal agents must only be used under medical supervision to avoid adverse effects.
References
- American Society for Reproductive Medicine (ASRM) – Practice Committee.
Testing and interpreting measures of ovarian reserve.
Official clinical guidelines by ASRM.
https://www.asrm.org - Bentov Y, Casper RF.
The aging oocyte—can mitochondrial function be improved?
Fertility and Sterility, Elsevier.
https://www.fertstert.org - Gleicher N, et al.
DHEA supplementation improves IVF outcomes in diminished ovarian reserve.
Human Reproduction, Oxford Academic.
https://academic.oup.com/humrep - European Society of Human Reproduction and Embryology (ESHRE).
Guideline on Ovarian Stimulation.
https://www.eshre.eu - Xu Y, et al.
Melatonin improves oocyte quality and embryo development.
Journal of Pineal Research, Wiley Online Library.
https://onlinelibrary.wiley.com
