
Vitamin B12 Deficiency and Heart Attack Risk: The Silent Danger Young Adults and Diabetics Must Know
Dr. Javed • May 24, 2026 • Cardiology & Nutrient
Heart Health Vitamin B12 Diabetes Homocysteine Prevention
Don’t ignore B12 — it’s vital for heart health. Vitamin B12 deficiency has quietly emerged as one of the most overlooked causes of heart attack, especially in young adults and diabetic patients. Here is everything you need to know.
The Hidden Epidemic: Why Vitamin B12 Deficiency Is More Dangerous Than You Think
Most people associate heart attacks with obesity, smoking, or high cholesterol. Yet cardiologists and endocrinologists worldwide are raising alarms about a far subtler threat: Vitamin B12 deficiency. This water-soluble vitamin, essential for nerve function and red blood cell formation, plays a critical and often underappreciated role in protecting your cardiovascular system.
When your body runs low on B12, a toxic amino acid called homocysteine accumulates in the bloodstream. Elevated homocysteine is now recognized as an independent risk factor for coronary artery disease — meaning it can cause plaque buildup and heart attacks all on its own, even in people with normal cholesterol levels and healthy weight. This is why Vitamin B12 deficiency deserves urgent medical attention.
39% of diabetics have clinically low B12 levels
2×higher heart attack risk with elevated homocysteine
6% of adults under 40 are B12 deficient
The Science: How Low B12 Leads Directly to Heart Attack
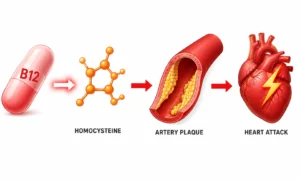
Understanding the mechanism behind Vitamin B12 deficiency and heart disease is straightforward once you follow the biochemical chain reaction. B12 is a key cofactor in the conversion of homocysteine into methionine — a harmless amino acid. When B12 is absent or insufficient, this conversion fails, and homocysteine levels surge.
Low B12
→
↑ Homocysteine builds up
→
Arterial wall damage
→
Coronary plaque forms
→
❤ Heart Attack
High homocysteine directly injures the endothelium — the delicate inner lining of your arteries. This injury triggers inflammation, oxidative stress, and the deposition of LDL cholesterol into the arterial wall, forming the dangerous plaques known as atherosclerosis. When those plaques rupture inside a coronary artery, the result is a myocardial infarction — a heart attack. This entire cascade begins silently with nothing more than Vitamin B12 deficiency.
Clinical Key Point Low Vitamin B12 → Elevated Homocysteine → Coronary Artery Plaque Formation → Heart Attack. This pathway is now well-documented in peer-reviewed cardiology literature and represents the most preventable cause of cardiovascular events in young and diabetic populations.
Why Young Adults Are the Most Vulnerable to Vitamin B12 Deficiency
Heart attacks in people under 40 were once considered medical rarities. Today, emergency cardiologists are seeing a troubling increase in young patients arriving with acute coronary syndromes — and a significant proportion have one thing in common: low serum B12. Several modern lifestyle factors drive Vitamin B12 deficiency in young adults:
- Vegetarian and vegan diets: B12 is found almost exclusively in animal products. Plant-based eaters who do not supplement are at very high risk of Vitamin B12 deficiency.
- Processed food habits: Ultra-processed diets crowd out nutrient-rich whole foods, leading to gradual depletion.
- Alcohol overuse: Alcohol impairs B12 absorption in the gut lining.
- Undiagnosed malabsorption: Conditions like celiac disease or atrophic gastritis silently reduce B12 uptake from food.
- Stress and gut health: Chronic stress alters gut flora and stomach acid, both critical for B12 absorption.
Because symptoms of Vitamin B12 deficiency — fatigue, mild cognitive fog, tingling in hands — are easy to dismiss as “stress” or “overwork,” young adults often go years without diagnosis. All the while, homocysteine climbs and arterial damage accumulates invisibly.
Diabetic Patients: Why Vitamin B12 Deficiency Is Doubly Dangerous
If you have diabetes — Type 1 or Type 2 — your risk of Vitamin B12 deficiency is dramatically elevated for two reasons that compound each other dangerously.
First: Metformin depletes B12. Metformin, the most widely prescribed diabetes medication in the world, is known to interfere with B12 absorption in the small intestine by blocking calcium-dependent receptors. Studies show that up to 30% of long-term Metformin users develop clinically significant Vitamin B12 deficiency — yet most are never screened for it.
Second: Diabetics already have elevated cardiovascular risk. High blood sugar independently damages blood vessels and promotes inflammation. When you add the homocysteine surge from Vitamin B12 deficiency on top of diabetic vascular injury, the risk of coronary artery plaque formation multiplies. A diabetic patient with undetected B12 deficiency is essentially accelerating their path toward a potentially fatal cardiac event.
For Doctors and Patients A like Current guidelines recommend monitoring B12 levels annually in all patients taking Metformin for more than 4 years. In practice, this check is frequently skipped. If you are a diabetic patient, proactively ask your physician to include serum B12 and homocysteine in your next blood panel.
Recognizing Vitamin B12 Deficiency: Warning Signs You Should Never Ignore
The insidious nature of Vitamin B12 deficiency lies in how long it can remain subclinical — causing internal damage while producing only vague or mild symptoms. Common warning signs include:
- Persistent fatigue and weakness that does not resolve with rest
- Tingling, numbness, or a “pins and needles” sensation in the hands, feet, or legs
- Pale or slightly jaundiced skin tone
- Shortness of breath and heart palpitations
- Memory difficulties or mental “fogginess”
- Glossitis — a sore, inflamed, or smooth red tongue
- Mood changes including depression or irritability
Critically, cardiovascular damage from elevated homocysteine caused by Vitamin B12 deficiency produces no distinct symptoms of its own until a cardiac event occurs. This is precisely why proactive blood testing — not symptom-watching alone — is the cornerstone of prevention.
Testing, Treatment, and Prevention of Vitamin B12 Deficiency
The good news is that Vitamin B12 deficiency is one of the most straightforward nutritional deficiencies to diagnose and treat. The following steps outline an evidence-based approach:
Testing: A simple blood test measuring serum B12 levels is the standard first-line diagnostic tool. Levels below 200 pg/mL are generally considered deficient, while levels between 200–300 pg/mL are borderline and warrant further investigation including plasma homocysteine and methylmalonic acid (MMA) measurement for confirmation.
Dietary sources: Animal products are the richest sources of B12. Include eggs, dairy, meat, poultry, and especially fish such as salmon, sardines, and tuna in your regular diet. For those following a plant-based diet, fortified foods — nutritional yeast, fortified plant milks, fortified cereals — and high-quality supplementation are non-negotiable to prevent Vitamin B12 deficiency.
Supplementation: Oral cyanocobalamin or methylcobalamin supplements are widely available and highly effective for most patients. In cases of malabsorption — such as pernicious anaemia or severe gut disease — intramuscular B12 injections bypass the digestive tract entirely and rapidly restore levels. Supplementation not only reverses Vitamin B12 deficiency but measurably reduces homocysteine levels within weeks, directly lowering cardiovascular risk.
Don’t Ignore B12
The relationship between Vitamin B12 deficiency and heart attack represents one of the most preventable tragedies in modern medicine. A cheap blood test, a dietary adjustment, or a daily supplement can interrupt a chain reaction that otherwise ends in a coronary care unit. Young adults should not assume they are immune to nutritional deficiencies. Diabetic patients on Metformin should insist on B12 monitoring. And everyone — regardless of age — should recognize that Vitamin B12 deficiency is not merely a fatigue issue or a nerve issue. It is a heart issue.
Speak to your physician today. Request a full metabolic panel that includes serum B12 and homocysteine. And remember: the heart you protect by addressing Vitamin B12 deficiency is your own.
FAQs
Q1: What is the connection between Vitamin B12 deficiency and heart attack?
Vitamin B12 deficiency leads to elevated homocysteine levels in the blood. High homocysteine damages the inner walls of arteries, promotes coronary plaque formation, and significantly increases the risk of a heart attack — even in young and otherwise healthy individuals.
Q2: Why are diabetic patients at higher risk of Vitamin B12 deficiency?
Diabetic patients are at higher risk for two reasons. First, Metformin — the most commonly prescribed diabetes medication — blocks B12 absorption in the gut. Second, diabetes already causes vascular inflammation, which compounds the arterial damage caused by low B12 and elevated homocysteine.
Q3: Can Vitamin B12 deficiency cause a heart attack in young people?
Yes. Vitamin B12 deficiency is now recognized as one of the most common and preventable causes of heart attack in young adults. Vegan and vegetarian diets, poor gut health, and alcohol use can all lead to B12 depletion and dangerously high homocysteine, triggering coronary artery disease at a young age.
Q4: How does low B12 increase homocysteine and damage arteries?
Vitamin B12 is essential for converting homocysteine into methionine. Without enough B12, homocysteine accumulates. High homocysteine injures the endothelium (the artery’s inner lining), triggering inflammation and LDL cholesterol deposition — the foundation of coronary artery plaques that can rupture and cause heart attacks.
Q5: What are the symptoms of Vitamin B12 deficiency to watch for?
Common symptoms include persistent fatigue, numbness or tingling in the hands and feet, pale skin, shortness of breath, heart palpitations, memory problems, and a sore or inflamed tongue. Importantly, the cardiovascular damage from B12 deficiency usually causes no symptoms until a cardiac event occurs.
Q6: How can I test for Vitamin B12 deficiency?
A simple blood test measuring serum B12 is the standard first-line test. Levels below 200 pg/mL indicate deficiency. For borderline results (200–300 pg/mL), doctors may also check plasma homocysteine and methylmalonic acid (MMA) levels for confirmation. Ask your physician to include these in your routine blood panel.
Q7: How can Vitamin B12 deficiency be treated to reduce heart attack risk?
Treatment depends on the cause. Oral B12 supplements (cyanocobalamin or methylcobalamin) are effective for most people. Those with malabsorption conditions may need intramuscular B12 injections. Dietary sources such as eggs, meat, fish, and dairy also help. Correcting B12 deficiency measurably lowers homocysteine within weeks, directly reducing cardiovascular risk.
Q8: Should people on Metformin routinely check their B12 levels?
Yes. Medical guidelines recommend annual B12 monitoring for patients who have been on Metformin for more than four years, though this is often skipped in practice. If you are a diabetic patient on Metformin, proactively request a serum B12 test from your physician at your next visit.
